German doctors report that teclistamab, a drug initially developed for multiple myeloma, significantly improved symptoms in two women suffering from severe autoimmune neuropathy that had resisted all standard treatments. Following just four injections, both patients showed disappearance of harmful antibodies, reduced nerve damage, and notable gains in walking ability, sensation, and daily functioning. The findings were published in Nature Communications.
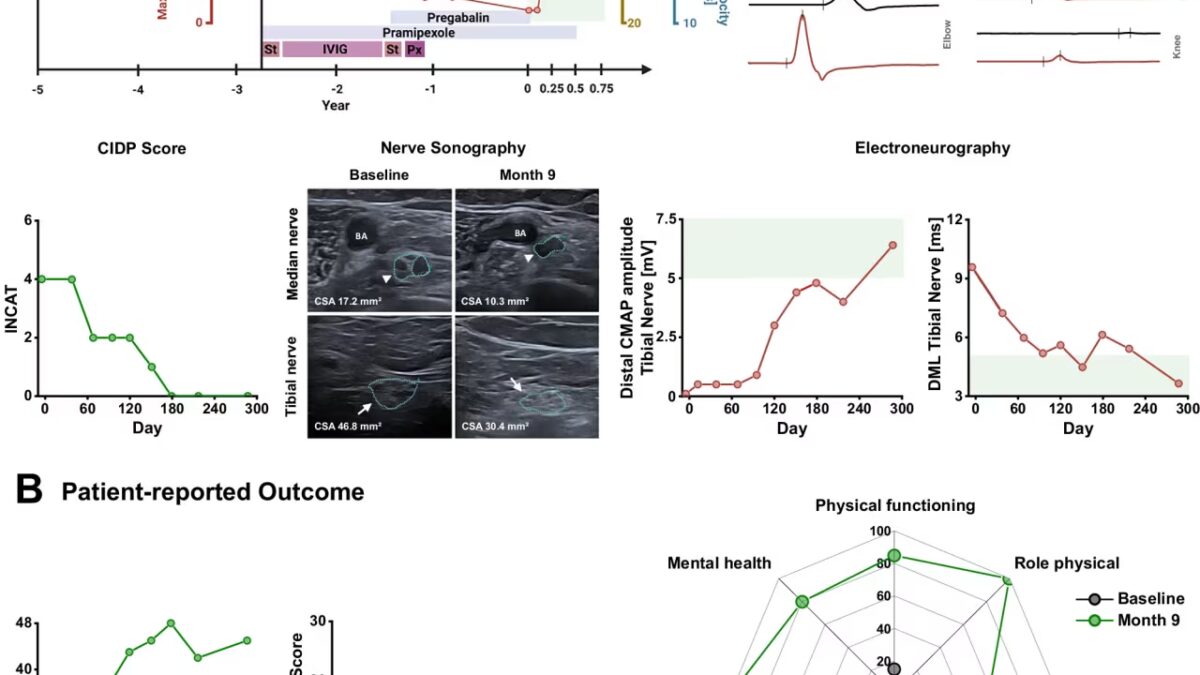
One of the patients, aged 73, had battled neuropathy for 13 years linked to antibodies against myelin-associated glycoprotein (MAG). Her condition briefly responded to steroids but then worsened relentlessly. Treatments including immunoglobulins, plasma exchange, and rituximab failed to halt disease progression. She developed ataxia, leg weakness, frequent falls, and fractures.
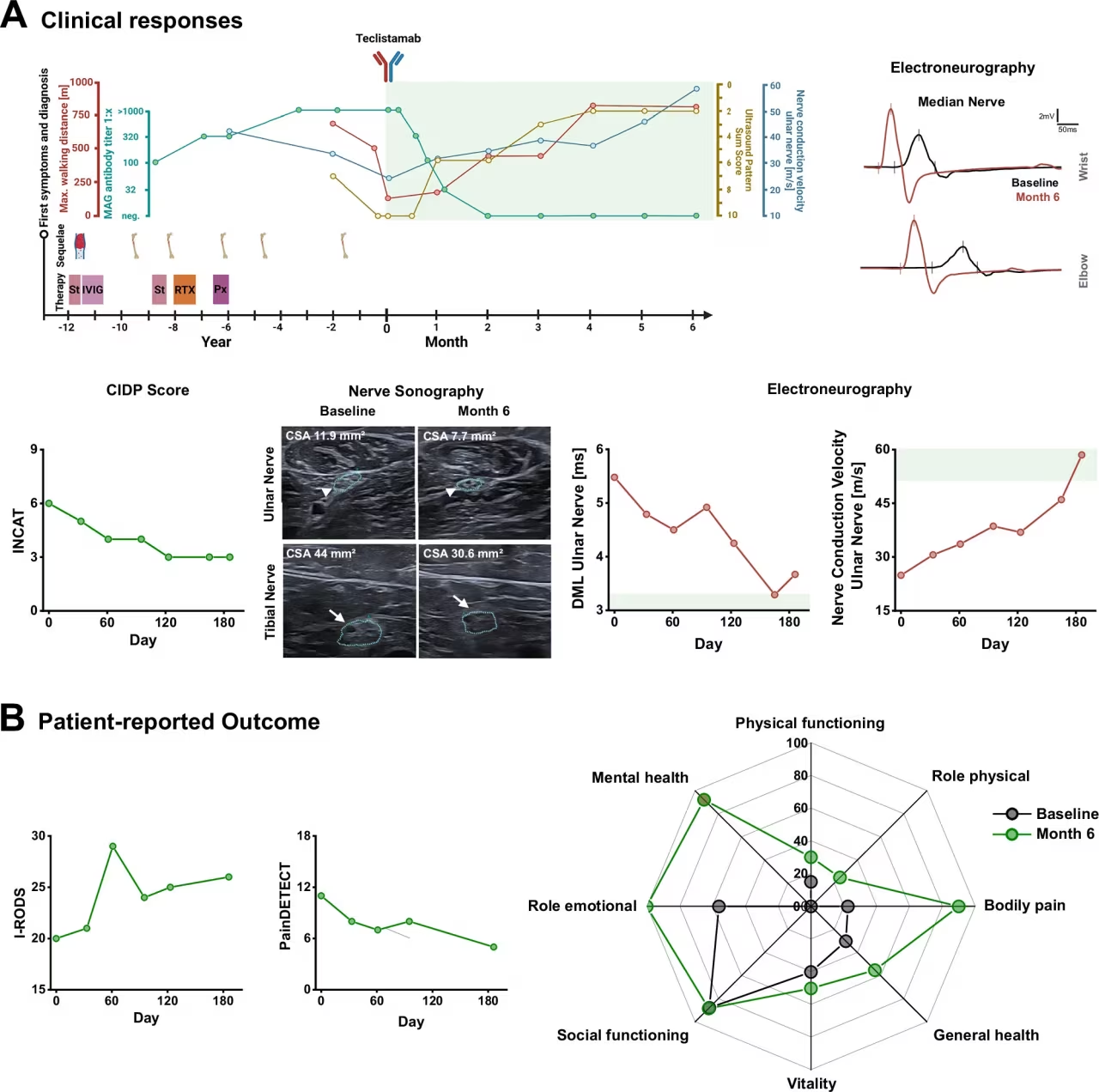
After the four-dose course of teclistamab, her walking distance increased more than sixfold within six months. Pain and neuropathy symptoms eased, quality of life improved, and tests revealed partial restoration of nerve conduction and decreased nerve swelling. Levels of paraprotein and anti-MAG antibodies dropped to undetectable, and neurofilament light chain – a marker of nerve damage – declined as well. Both patients experienced only moderate, manageable side effects.
Teclistamab’s potential for autoimmune neuropathy treatment
Teclistamab is an immunotherapy designed to target and eliminate B cells and plasma cells – the antibody-producing culprits often responsible for multiple myeloma. Its success in these neuropathy cases marks an intriguing crossover from cancer treatment to neurology, especially since conventional immunotherapies had failed. The researchers noted that B cells initially vanished after the treatment but later repopulated predominantly as naive cells, hinting at an immune system ”reset” rather than merely a temporary suppression of inflammation.
This approach is part of a growing trend where hematology-oncology therapies find new roles in neuroimmunology. Previously, a German team reported two severe autoimmune polyneuropathy patients who regained mobility after receiving CAR-T cell therapy. Compared to CAR-T, teclistamab offers a simpler option since it is an off-the-shelf drug rather than customized cell therapy.
However, caution is warranted. The published evidence covers only two cases, and chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) and related disorders remain rare – affecting just a few dozen per 100,000 people – with treatment-resistant forms being even scarcer. Still, such isolated successes draw attention for patients with no other viable options.
Teclistamab’s established use in multiple myeloma – where it engages T cells to kill malignant plasma cells – gives it a practical edge over experimental treatments like CAR-T therapy, which requires individualized manufacturing and carries substantial costs. This positions teclistamab as a potentially accessible option for neurologists tackling stubborn autoimmune nerve diseases.
Future larger clinical trials will be essential to determine how reproducible these effects are across more patients and how durable the benefits remain after a short treatment course. If supported by further evidence, teclistamab could become a valuable addition to the limited toolkit for treating refractory autoimmune neuropathies that defy existing therapies.